Chez les patients présentant un infarctus du myocarde avec élévation du segment ST (STEMI), une intervention coronaire percutanée de la lésion coupable réduit le risque de mort cardiovasculaire ou d’infarctus du myocarde. Dans le travail présenté dans ce nouvel article que signent des partenaires de iVASC, il est montré que pratiquer une intervention coronaire percutanée ‘complète‘ sur des lésions non-coupables quand les patients présentaient une maladie coronaire multivaisseaux réduit significativement le risque cardiovasculaire.
Mehta SR, Wood DA, Storey RF, Mehran R, Bainey KR, Nguyen H, Meeks B, Di Pasquale G, Lopez-Sendon J, Faxon DP, Mauri L, Rao SV, Feldman L, Steg PG, et al for the COMPLETE Trial Steering Committee and Investigators
Complete Revascularization with Multivessel PCI for Myocardial Infarction
N Engl J Med 2019. PubMed
BACKGROUND
In patients with ST-segment elevation myocardial infarction (STEMI), percutaneous coronary intervention (PCI) of the culprit lesion reduces the risk of cardiovascular death or myocardial infarction. Whether PCI of nonculprit lesions further reduces the risk of such events is unclear.
METHODS
We randomly assigned patients with STEMI and multivessel coronary artery disease who had undergone successful culprit-lesion PCI to a strategy of either complete revascularization with PCI of angiographically significant nonculprit lesions or no further revascularization. Randomization was stratified according to the intended timing of nonculprit-lesion PCI (either during or after the index hospitalization). The first coprimary outcome was the composite of cardiovascular death or myocardial infarction; the second coprimary outcome was the composite of cardiovascular death, myocardial infarction, or ischemia-driven revascularization.
RESULTS
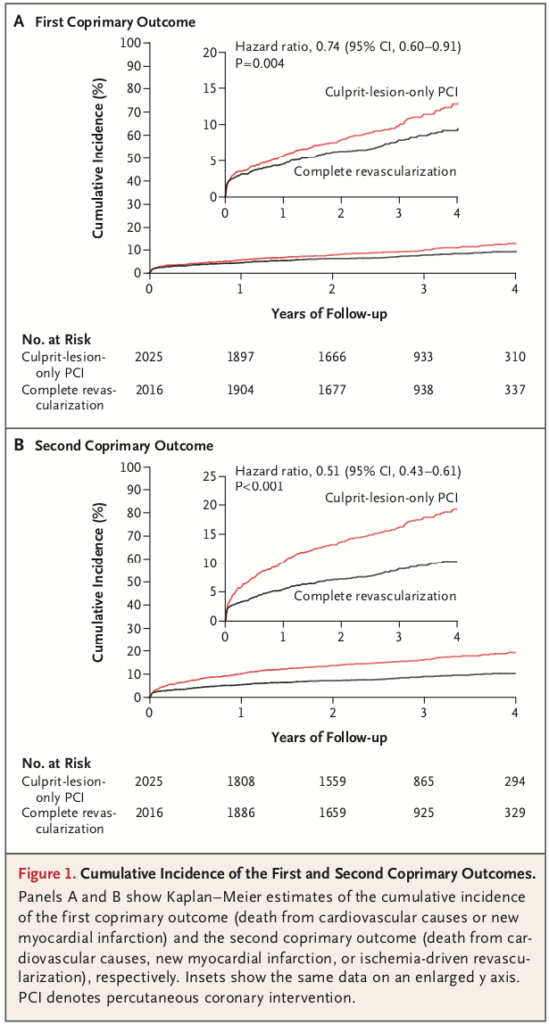
At a median follow-up of 3 years, the first coprimary outcome had occurred in 158 of the 2016 patients (7.8%) in the complete-revascularization group as compared with 213 of the 2025 patients (10.5%) in the culprit-lesion-only PCI group (hazard ratio, 0.74; 95% confidence interval [CI], 0.60 to 0.91; P = 0.004). The second coprimary outcome had occurred in 179 patients (8.9%) in the complete-revascularization group as compared with 339 patients (16.7%) in the culprit-lesion-only PCI group (hazard ratio, 0.51; 95% CI, 0.43 to 0.61; P<0.001). For both coprimary outcomes, the benefit of complete revascularization was consistently observed regardless of the intended timing of nonculprit-lesion PCI (P = 0.62 and P = 0.27 for interaction for the first and second coprimary outcomes, respectively).
CONCLUSIONS
Among patients with STEMI and multivessel coronary artery disease, complete revascularization was superior to culprit-lesion-only PCI in reducing the risk of cardiovascular death or myocardial infarction, as well as the risk of cardiovascular death, myocardial infarction, or ischemia-driven revascularization. (Funded by the Canadian Institutes of Health Research and others; COMPLETE ClinicalTrials.gov number, NCT01740479.).